



The
axillary nerve
The axillary nerve arises from the posterior
cord of the brachial plexus and has a root value of C5, 6. In the axilla it
descends behind the axillary artery and in front of subscapularis, at the lower border of which it passes backwards
close to the inferior part of the shoulder joint in company with the posterior
circumflex humeral vessels. It then passes through the quadrilateral space where it supplies the shoulder joint and
divides into anterior and posterior branches. The anterior branch winds around
the surgical neck of the humerus,
deep to and as far as the anterior part of deltoid,
which it supplies. The posterior branch supplies teres minor, and the posterior part of deltoid. It then passes around deltoid
as the upper lateral cutaneous nerve of
the arm which pierces the deep fascia to supply skin over the lower part of
deltoid and the lateral head of triceps as far as the middle part of the
arm.
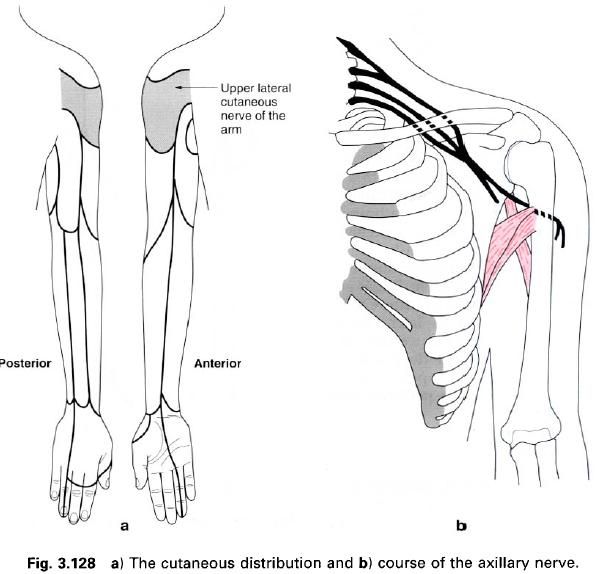
The axillary nerve is frequently injured when
the shoulder is dislocated because of
its close proximity to this joint. Paralysis of deltoid and teres minor results, and consequently there is inability to abduct the arm beyond that
possible by the action of supraspinatus.
This, in conjuction with an area of anaesthesia over the back of deltoid and lateral head of triceps, allows a clinical diagnosis of
nerve injury to be made.
The
musculocutaneous nerve
The musculocutaneous nerve arises from the
lateral cord of the brachial plexus and has a root value C5, 6, 7. It lies
firstly lateral to the axillary artery and then descends between the artery and
coracobrachialis which it supplies
and pierces before running distally between biceps and brachialis to reach the
lateral side of the arm. At the elbow, the musculocutaneous nerve pierces the deep
fascia between biceps and brachioradialis as the lateral cutaneous nerve of the forearm.
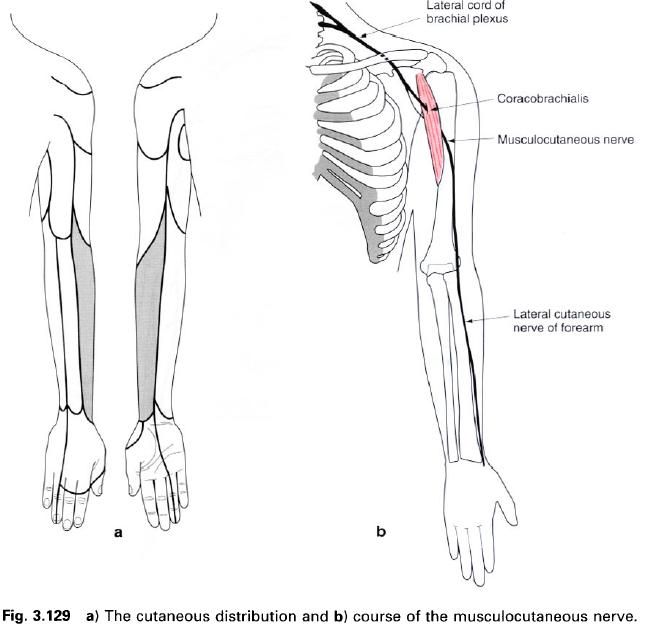
In the arm the musculocutaneous nerve supplies
both heads of biceps brachii and
two-thirds of brachialis as well as coracobrachialis.
The
lateral cutaneous nerve of the forearm divides into anterior and posterior branches. The anterior branch
supplies the skin on the lateral half of the forearm as far as the ball of the
thumb, while the posterior branch supplies a variable area over the extensor
muscles of the forearm, wrist and occasionally the first metacarpal.
The
ulnar nerve
The ulnar nerve is one of the terminal branches
of the medial cord of the brachial plexus, having a root value C8 and T1, but
frequently contains fibres from C7. It descends on the medial side of the
axillary artery behind the medial cutaneous nerve of the forearm, and continues
downwards medial to the brachial artery, anterior to triceps. In the distal half of the arm, the ulnar nerve passes
backwards and pierces the medial intermuscular septum to enter the posterior
compartment of the arm, where it lies on the front of the medial head of triceps. Continuing its descent in the
posterior compartment of the arm, the ulnar nerve passes between the medial
epicondyle of the humerus and the olecranon
of the ulna, lying in the ulnar
groove behind the medial epicondyle. The ulnar nerve then enters the anterior
compartment of the forearm by passing between the two heads of flexor carpi ulnaris, initially in
contact with the ulnar collateral ligament of the elbow. As it descends along
the medial side of the forearm, the ulnar nerve lies on flexor digitorum profundus, lateral to the ulnar artery, covered in
its upper part by the belly of flexor carpi ulnaris, but in the lower half, only by its tendon. Proximal to the
flexor retinaculum it pierces the deep fascia to lie lateral to flexor carpi ulnaris, and passes
anterior to the flexor retinaculum lateral to the pisiform where it divides
into superficial and deep branches.
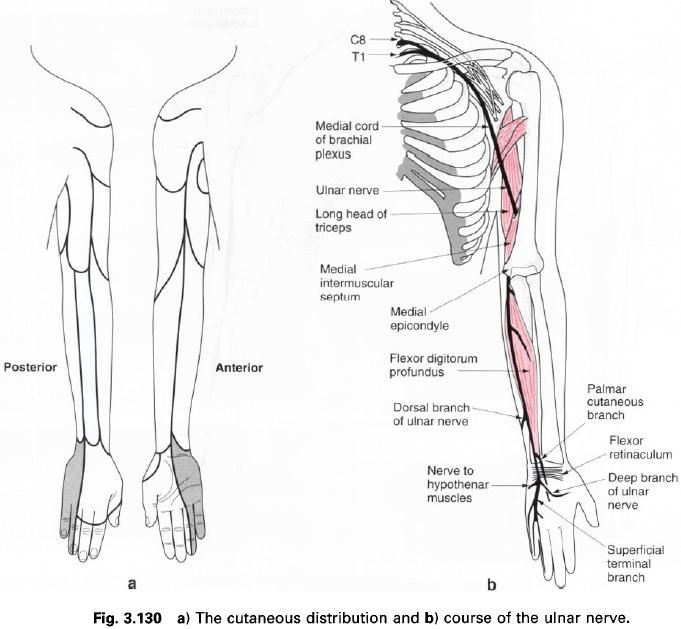
During its course, the ulnar nerve gives an
articular branch to the elbow joint, and supplies flexor carpi ulnaris, and the medial half of flexor digitorum profundus.
A
palmar cutaneous branch arises
from the ulnar nerve piercing the deep fascia in the distal third of the
forearm and descends to supply the skin over the medial part of the palm.
The dorsal
branch of the ulnar nerve also arises in the distal third of the forearm,
passes backwards deep to flexor carpi ulnaris to pierce the deep fascia on the medial side to become superficial.
On the medial side of the wrist, it crosses the triquetral, against which it
can be palpated, and gives branches to the dorsal surface of the wrist and hand. Here it divides into two or three
dorsal digital nerves which supply the skin on the dorsum of the hand and the dorsal surfaces of the
medial one and a half or two and a half fingers, excluding the skin over the
distal phalanx. The dorsum of the distal phalanges is supplied by branches from
the median or ulnar nerves derived from the palm.
The
superficial branch of the ulnar nerve lies deep to palmaris brevis
on the medial side of the hand where
it can be compressed against the hook of the hamate. It supplies the palmaris brevis muscle, the skin on the
medial side of the palm of the hand,
and the skin on the palmar surface of the little and adjacent half of the ring
fingers, extending onto the dorsal surface supplying the skin and nail bed of
the distal phalanx.
The
deep branch of the ulnar nerve
eventually runs with the deep branch of the ulnar artery and thus loops across
the palm from medial to lateral deep to the flexor tendons. It passes initially
between abductor digiti minimi and flexor digiti minimi and pierces opponens digiti minimi, supplying all
three muscles. As it passes across the deep part of the palm, it supplies the
medial two lumbricals, all of the interossei
and adductor pollicis. Rarely, the
ulnar nerve also supplies the thenar muscles. The deep branch gives articular
filaments to the wrist joint.
Applied
anatomy
The ulnar nerve may be damaged in the groove
behind the medial epicondyle either by trauma or entrapment. This leads to a
partial of complete loss of muscular and sensory innervation. At the wrist, the
nerve can easily be cut or lacerated because of its superficial position. The
clinical picture can be complicated if the lesion occurs below the level where
the dorsal and palmar cutaneous branches are given off, as a considerable
portion of the skin on the ulnar side of the hand still has a sensory supply.
The result of an ulnar nerve lesion often gives the typical “claw-hand
deformity”.
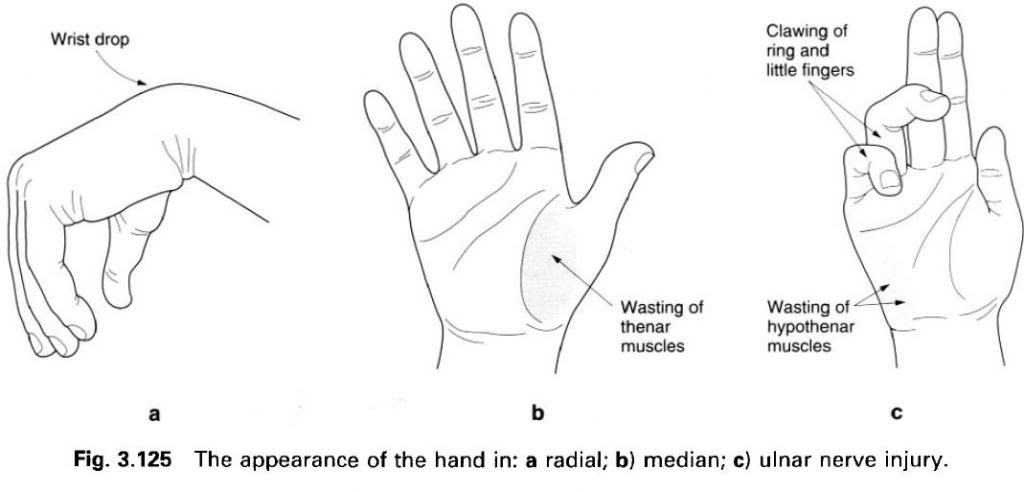
This is due to loss of power in the intrinsic
muscles of the hand and the unopposed
actions of antagonistic muscle groups. There is “guttering” between the
metacarpals, an inability to abduct the fingers or adduct the thumb. The area
of sensory loss usually follows the outline of the sensory map.










0 коментара:
Постави коментар